Laparoscopic excision of Bilateral Large Endometriomas in a young Nulligravida
A 24-year-old lady presented to us 6 months after marriage with severe pain during menses. An ultrasound examination revealed large endometriotic cysts of around 8 x 6 cms in both her ovaries. The patient and her husband were counseled and worked up extensively. Her ovarian reserve was assessed through sonography and blood tests. Her menstrual cycles were regular.
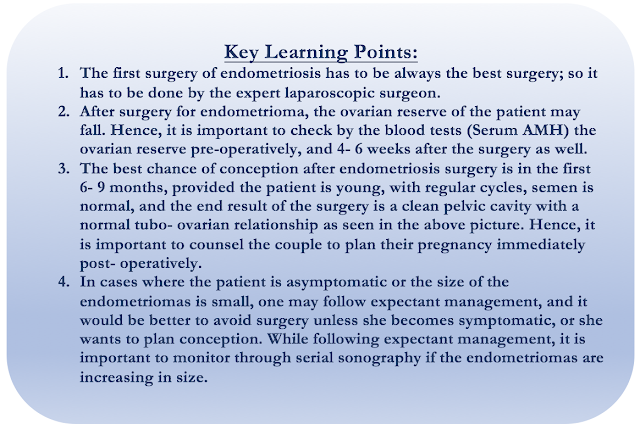
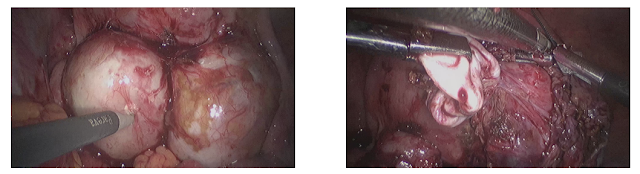
Considering her young age and symptomatic nature, the large size of endometriotic cysts, a decision to perform laparoscopic surgery to remove the endometriotic cysts was taken. Intra-operatively, extensive endometriosis was seen, with pelvic adhesions and endometriotic spots extending up to the upper abdomen, anterior abdominal wall, and subdiaphragmatic area.
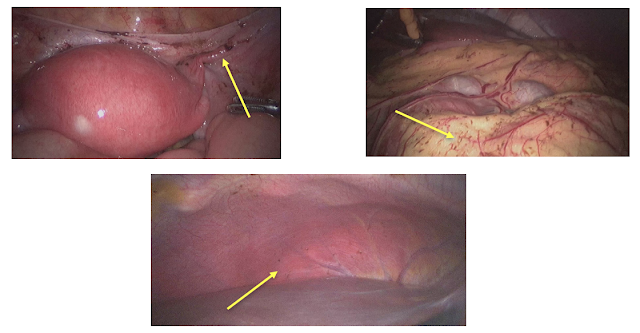
Bilateral endometriomas were seen with posterior adhesions to uterosacral ligaments. The course of the ureters was traced, and care taken to avoid damage to them. A novel method of enucleation of endometriotic cysts was followed. Vasopressin, in a dilution of 1: 150 was instilled in the peri- cystic area of the endometrioma, within the capsule. This helped in delineating the plane of dissection and making it less vascular during enucleation. The incision was taken over the capsule, and the intact cyst was enucleated by the traction- counter traction method.

Principles of surgery are adhered to while performing the laparoscopic endometriotic cystectomy.
The advantage being, that the Endo- ART Surgeons always have an edge, since they know how important it is to preserve the normal ovarian tissue, while at the same time, to perform a complete surgery to prevent a recurrence.
Endometriotic cysts are known to be highly vascular, more so at the base. However, care was taken that cautery was used always on the cyst wall and not the ovarian tissue, so as to minimize the damage to the normal ovary.
The specimen was retrieved in an endo-bag, so as to avoid port site endometriosis in the future.
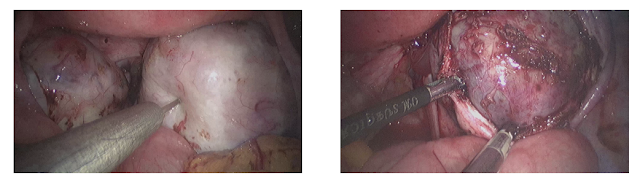
A thorough peritoneal and pelvic lavage was given. It is important to leave a clean pelvic cavity as the end result, so as to prevent the formation of adhesions.
Laparoscopic excision of Multiple Bilateral Endometriomas in a young woman with primary infertility
A 24-year-old nulligravida came to us with primary infertility of 1.5 years’ duration. She has regular cycles; her husband’s semen analysis was normal. However, on a transvaginal ultrasound done in the clinic, multiple bilateral endometriomas were noted.
Her AMH was 1.55, and the other investigations within normal limits.
Considering her young age, and multiple endometriomas, anxiety to conceive, laparoscopic excision of bilateral endometriomas was done.
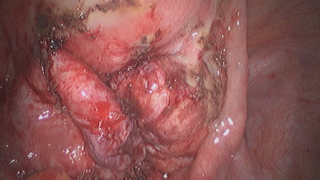
Intraoperatively, bilateral ovaries were seen enlarged and adherent to the posterior uterine wall and Pouch of Douglas.
The course of ureters was traced bilaterally and care was taken to avoid damage to them. In the case of endometriosis, the ureters may be pulled medially, and it is important that one visualizes them and avoids damage to them.
The incision was taken individually on the surface of the endometriomas, and chocolate-colored fluid was drained. The cyst wall was enucleated using the traction- counter traction method. Two endometriomas (3 x 2 cms each) were removed from the left ovary and four (2 x 2 cms each) from the right.
Principles of surgery were adhered to. Care was taken to avoid damage to the normal ovarian tissue, while, at the same time, completeness of the surgery was ensured.
Endometriomas are known to be highly vascular, especially at the base. However, cautery was used only on the cyst wall if necessary, and not on the ovarian tissue to prevent damage to it. Minimal use of cautery on the raw areas was done. Hemostasis was ensured by compression, and by the use of hemostatic solution (Hemlock).
Being an Endo- ART specialist, one can ensure that the surgery is performed with absolute finesse and care.
It is important to leave behind an absolutely clean pelvic cavity, and give a thorough pelvic lavage, so as to minimize post-operative adhesions.