What is a fibroid/myoma?
Fibroids or myomas or leiomyoma are non cancerous smooth muscle cell tumours arising from the wall of the uterus which are the commonest benign gynecologic tumour seen in 20-50% of women of reproductive age.
What are the different types of fibroids/myomas?
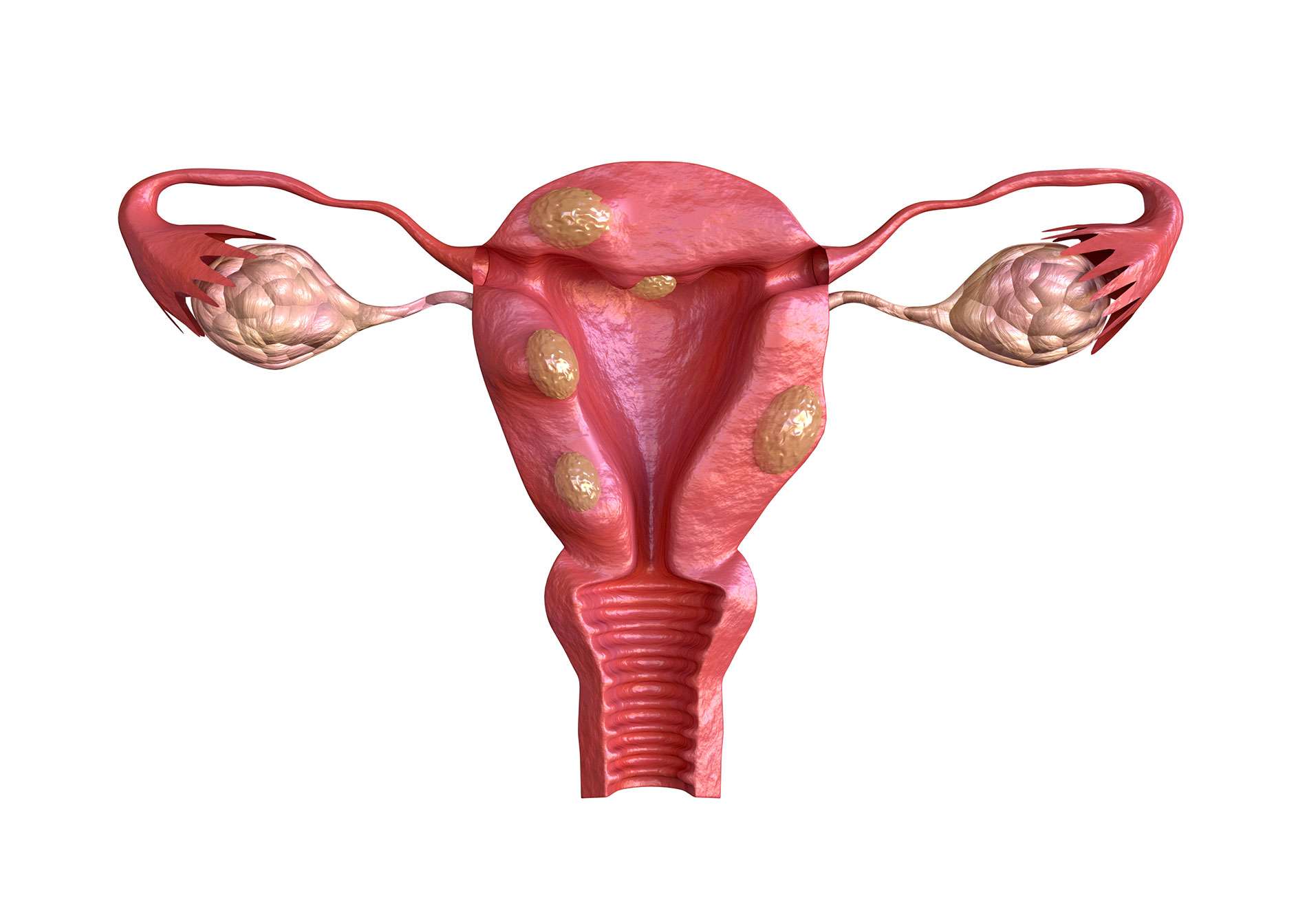
There are three main types of fibroids based on their location in the uterine wall. Although all fibroids primarily originate from the middle layer of the uterus i.e. the myometrium they are classified further as follows-
- Submucosal fibroids: Grow into and distort the cavity of the uterus.
- Intramural fibroids: Grow in the muscle wall of the uterus without distorting the cavity.
- Subserosal fibroids: Grow on the outer most lining of the uterus away from the cavity.
What are the symptoms of fibroid?
Symptoms vary depending upon the size and location of the myoma.
A patient with fibroids may have the following complaints:
- Changes in menstruation pattern:
—Longer, more frequent, or heavy menstrual periods
—Menstrual pain (cramps)
—Vaginal bleeding at times in between menstrual cycles
- Pain
—In the abdomen or lower back (usually dull, heavy and aching)
—During sex or menses.
- Pressure
—Difficulty urinating or frequent urination
—Constipation
—Abdominal cramps
- Enlarged uterus and abdomen
- Recurrent miscarriages
- Infertility
How do fibroids cause infertility?
- Submucous myomas may act as intrauterine devices and produce subacute endometritis leading to failure of implantation.
- Intramural myomas occurring in the region of the tubal ostia may cause tubal blockage.
- Compression and dilatation of adjacent vasculature may cause abnormal endometrial maturation, which may be inhospitable for embryo maturation.
- Large intramural, submucous or the combined variety of myomas may cause atrophic or ulcerated endometrium, which is hostile to nidation.
- Distortion of the endometrial cavity may increase the travel distance for the sperm.
- Prostaglandins present in the seminal plasma are believed to increase rhythmic myometrial contractility possibly facilitating sperm transport. Myomas in some way interfere with this mechanism and may decrease fertilization rates.
- Changes in the endometrium mediated by inflammation and factors involved in the process of fibrosis could also have a detrimental effect. In addition, fibroids may affect gene expression patterns in the endometrium (such as HOXA10), disrupting the window of implantation.
- Distort the uterus- making it enlarged, elongated, alters its contour and surface area
- This can impair the migration of sperm/ ovum/ embryo and also negatively impact implantation
- Dysfunctional and altered uterine contractility could hinder gamete and embryo transportation
- Affect overlying endometrium, creating endometrial vascular disturbances, inflammation, thinning, altered biochemical ch again can impair implantation
When is treatment necessary for fibroids?
Most fibroids may not cause any symptoms at all and maybe diagnose during a routine pelvic examination. Such fibroids that are small, asymptomatic and diagnosed near menopause don’t require treatment. However, fibroids are associated with any of the above symptoms which are severe enough to disrupt a patients daily activities, those affecting the fertility or IVF results (Implantation) or repeated miscarriage or those with rapid growth and uncertainty regarding their origin need to be investigated and treated.
Can medication be used to treat fibroids?
Drug therapy is an option for some women with fibroids. Although fibroids cannot be eliminated by medications they can be used to provide symptomatic relief. Surgery often is needed later. Various combined birth control pills, Gonadotropin-releasing hormone (GnRH) agonists, Progestin–releasing intrauterine devices; NSAIDs have been used for symptomatic treatment.
What types of surgery may be done to treat fibroids?
Fibroids may be treated surgically in two ways.
- Myomectomy: – This is the surgical removal of only fibroids while leaving the uterus in place. As the woman retains her uterus, she may still be able to have children. Fibroids do not regrow after such s surgery, but new fibroids may develop requiring treatment.
- Hysterectomy is the removal of the uterus. The ovaries may or may not be removed. Hysterectomy is done when other treatments have not worked or are not possible or the fibroids are very large. A woman is no longer give birth to a child after having a hysterectomy.
Both procedures can be performed either endoscopically or the more conventional open technique.
What is an endoscopic approach and which is better – Endoscopic or open?
The endoscopic approach involves the use of a camera attached to an endoscope, which is used to visualize the fibroid and surgically remove it. It can be of two types:
- Hysteroscopic myomectomy: This technique is used to remove submucosal fibroids that protrude into the cavity of the uterus. A resectoscope is inserted through the hysteroscope. The resectoscope destroys fibroids with electricity or a laser beam. This is an outpatient surgical procedure and patients can go home the same day of surgery with minimal side effects. Larger fibroids may require more than one sitting for removal.
- Laparoscopic approach: This approach involves making small 0.5-1 cm incisions on the abdominal wall through which the surgery is performed using a camera for visualization. In the hands of an expert, a laparoscopic approach is definitely preferred and can be used for almost all patients with fibroids barring a few. It is associated with a quicker recovery, less postoperative pain, and less febrile morbidity. Patients typically go home the day of or the day after their surgery.


