Antenatal Care in India: What Every Appointment Should Include
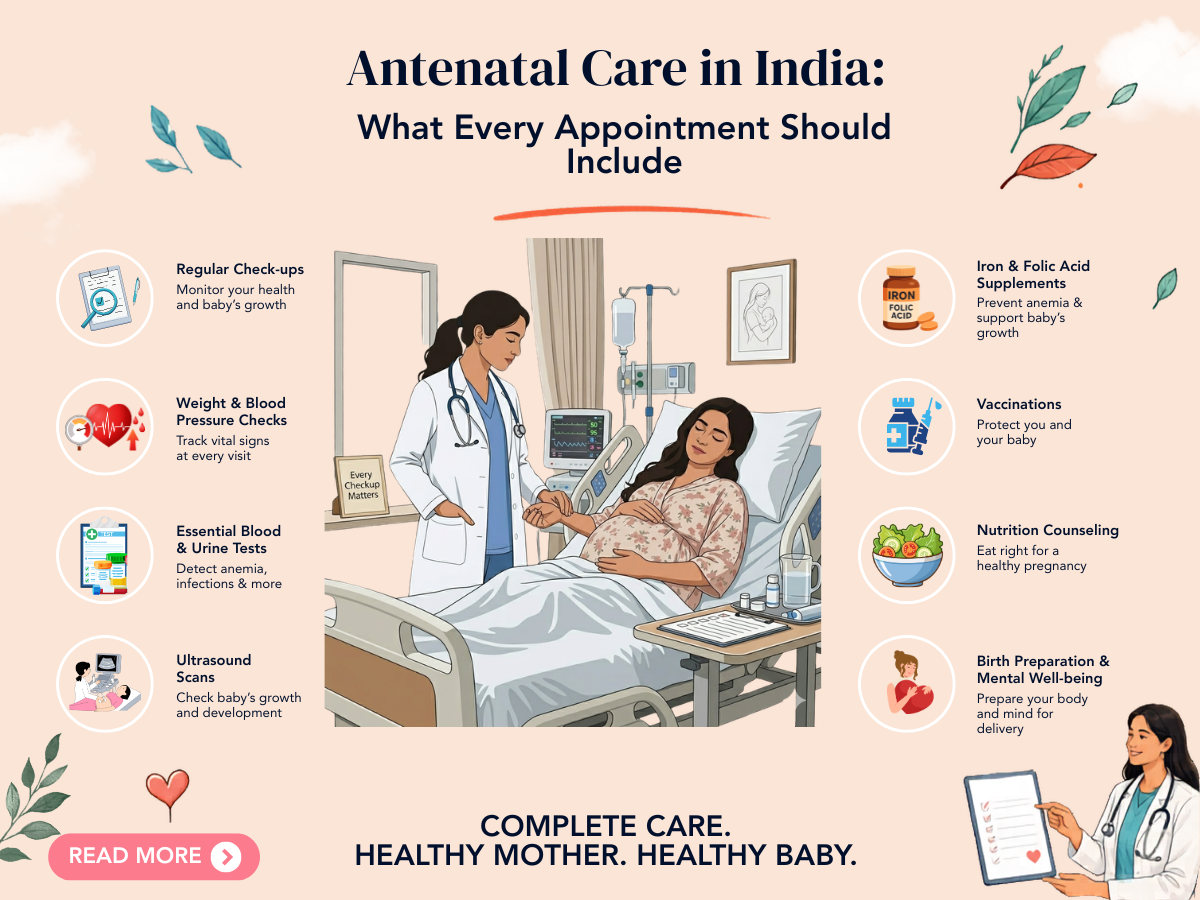
Antenatal care — the systematic medical monitoring of pregnancy from confirmation of pregnancy to delivery — is one of the most evidence-based interventions in medicine. Its purpose is to identify problems early enough to act on them effectively, to provide education and support that empowers women to manage their own health during pregnancy, and to plan for a safe delivery. Yet across India, the quality and completeness of antenatal care varies dramatically — from excellent comprehensive monitoring in well-resourced urban centres to minimal or absent care in underserved areas.
This guide explains what good antenatal care looks like — appointment by appointment — so that pregnant women in India know what to expect and what to ask for.
First Trimester: Establishing the Foundation (Weeks 6 to 12)
First Appointment — 8 to 10 Weeks (or Earlier for IVF or High-Risk)
The first antenatal appointment is the most comprehensive of all. It should include:
- Confirmation and dating of the pregnancy: Either by last menstrual period if cycles are regular, or by early ultrasound (the most accurate method for dating).
- Comprehensive medical and obstetric history: Previous pregnancies, miscarriages, medical conditions, medications, family history of genetic conditions.
- Physical examination: Blood pressure, weight, BMI, assessment for any clinical abnormality.
- Booking blood tests: Blood group and Rh status, full blood count, blood glucose, thyroid function (TSH), rubella immunity, VDRL, HIV, hepatitis B surface antigen, hepatitis C antibody. Haemoglobin electrophoresis if relevant family history.
- Urine culture: To detect asymptomatic bacteriuria — untreated in pregnancy it significantly increases risk of pyelonephritis and preterm birth.
- First trimester combined screening: Nuchal translucency ultrasound (at 11 to 13+6 weeks) combined with maternal blood tests (free beta-hCG and PAPP-A) — screen for trisomy 21 (Down syndrome), 18, and 13.
- NIPT (Non-Invasive Prenatal Testing): Can be offered from 10 weeks — a blood test detecting foetal chromosomal DNA in maternal blood. More accurate than combined screening. Offered to all; strongly recommended for advanced maternal age (above 35), IVF pregnancies, and previous chromosomal anomaly.
- Prescriptions: Folic acid (if not already started), iron and calcium supplementation if indicated, aspirin 75 to 150 mg if high-risk for pre-eclampsia.
Second Trimester: Surveillance and Screening (Weeks 14 to 28)
16 to 18 Weeks
- Blood pressure and urine protein
- Foetal heart auscultation
- Assessment of gestational diabetes risk — early OGTT for high-risk women (previous GDM, PCOS, BMI above 30, family history of diabetes)
- Cervical length measurement (transvaginal ultrasound) for women at elevated preterm risk
18 to 20 Weeks — Anomaly Scan
The detailed foetal anatomy scan — the most important ultrasound of the pregnancy. A thorough scan at 18 to 20 weeks assesses:
- Foetal anatomy: Head (brain structure, face, lip), chest (heart, lungs), abdomen (stomach, kidneys, bladder, abdominal wall), spine, limbs
- Placental location and appearance
- Amniotic fluid volume
- Foetal growth measurements
A detailed cardiac views assessment is part of the standard anomaly scan. If the sonographer is not confident, a repeat scan with a foetal medicine specialist is appropriate.
24 to 28 Weeks
- Universal gestational diabetes screening: 75g OGTT for all pregnant women not yet screened
- Full blood count: To detect gestational anaemia
- Blood pressure and urine protein: Pre-eclampsia surveillance
- Anti-D immunoglobulin: For Rh-negative women (at 28 weeks, and again at 34 weeks in some protocols)
Third Trimester: Intensified Monitoring (Weeks 28 to 40+)
28 to 32 Weeks
- Growth scan: Foetal measurements to assess growth velocity and amniotic fluid
- Uterine artery and umbilical artery Doppler (for women with pre-eclampsia risk or growth restriction)
- Blood pressure and urine protein — more frequent in high-risk pregnancies
- Repeat full blood count
32 to 36 Weeks
- Group B Streptococcus (GBS) vaginal/rectal swab: GBS is found in approximately 20 to 25% of women and — if present during labour — can cause serious neonatal infection. IV antibiotics in labour prevent transmission. Increasingly offered in Indian high-risk antenatal care.
- Discussion of birth plan, delivery preferences, and signs of labour
36 to 40 Weeks
- Foetal presentation (head-down or breech) — if breech at 36 weeks, external cephalic version (ECV) may be offered
- Growth and wellbeing scan
- Cervical assessment for delivery planning
- Discussion of when to seek emergency assessment (signs of labour, reduced movements, bleeding, severe headache or visual changes)
What Good Antenatal Care Should Always Include
- Blood pressure measurement at every visit — the cornerstone of pre-eclampsia surveillance
- Urine dipstick for protein at every visit
- Foetal heart auscultation at every visit from 12 weeks onward
- Weight measurement and tracking
- Answers to questions — every appointment should include time for the pregnant woman to ask questions and receive clear, understandable answers
- A clear, documented plan — the woman should always leave knowing what will happen at the next appointment and what to do if she has concerns in between
Frequently Asked Questions
Q1. How often should I attend antenatal appointments in a normal pregnancy?
In a low-risk pregnancy, approximately 8 to 10 appointments throughout the pregnancy are recommended — roughly monthly in the first and second trimesters, fortnightly in the third trimester from 28 to 36 weeks, and then weekly approaching term. High-risk pregnancies require more frequent monitoring — the specific schedule depends on the risk factors present.
Q2. My antenatal provider is not measuring my cervical length. Should they be?
Universal cervical length measurement is not standard in all low-risk singleton pregnancies. It is recommended for women at elevated preterm risk (previous preterm birth, previous second-trimester loss, previous cone biopsy or LLETZ, twin pregnancy). If you have any of these risk factors and cervical length has not been measured, ask specifically for this assessment.
Q3. Is it okay to change obstetricians mid-pregnancy?
Yes — you can change obstetricians at any point in pregnancy. Bring all your previous appointment records, blood test results, ultrasound reports, and any previous pregnancy history to the new provider. The most important thing is that your care is appropriately monitored — a change in provider should not result in missed screening or surveillance. The new provider will need to review all previous investigations to ensure the monitoring programme is current and complete.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Every pregnancy is unique. Please consult Dr. Sunita Tandulwadkar or your qualified obstetrician for personalised guidance. Solo Clinic IVF & ObGyn, Pune