Pre-Eclampsia: Warning Signs Every Pregnant Woman in India Should Know
Pre-eclampsia is one of the most serious complications of pregnancy — a leading cause of maternal death and preterm birth globally, and a significant contributor to maternal and perinatal mortality in India. Despite its severity and its preventability in many cases, a large proportion of Indian women do not know what pre-eclampsia is, what its warning signs are, or when to seek urgent care.
This article provides the clear, plain-language information that every pregnant woman in India deserves about pre-eclampsia — including how to recognise it, what increases risk, and how early detection and treatment save lives.
What Is Pre-Eclampsia?
Pre-eclampsia is a pregnancy-specific disorder characterised by new-onset hypertension (blood pressure of 140/90 mmHg or higher) developing after 20 weeks of gestation, combined with proteinuria (protein in the urine) or evidence of end-organ dysfunction — involving the liver, kidneys, brain, or placenta.
It is not simply "high blood pressure in pregnancy." Pre-eclampsia is a systemic disease originating from abnormal placentation — a failure of the spiral arteries that supply the placenta to remodel properly in early pregnancy. This leads to a cascade of vascular inflammation, endothelial dysfunction, and end-organ damage that can threaten multiple organ systems simultaneously.
Untreated severe pre-eclampsia can progress to:
- Eclampsia: Seizures — a life-threatening emergency
- HELLP syndrome: Haemolysis, Elevated Liver enzymes, Low Platelets — a severe variant affecting the blood and liver
- Pulmonary oedema: Fluid in the lungs
- Acute kidney injury
- Placental abruption
- Intrauterine foetal compromise or death
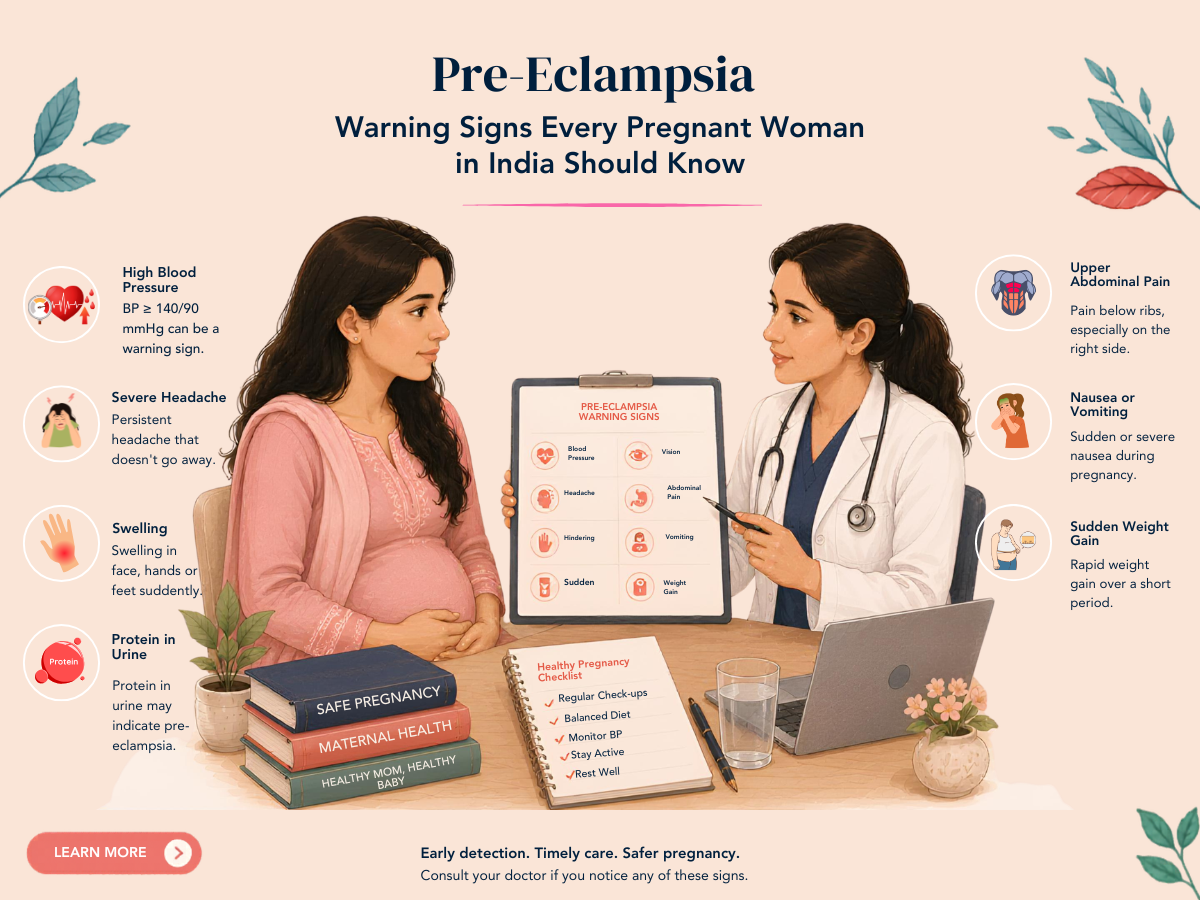
Warning Signs Every Pregnant Woman Should Know
After 20 weeks of pregnancy, the following symptoms should prompt immediate contact with the obstetrician or emergency services — they are not "normal" pregnancy discomforts:
- Severe headache that does not respond to paracetamol — particularly at the front or back of the head
- Visual disturbances: flashing lights, blurring, blind spots, or temporary vision loss
- Sudden severe swelling of the hands, face, or feet — particularly if asymmetric or rapidly worsening
- Upper abdominal pain or tenderness — particularly under the right rib cage (liver area) or in the epigastrium
- Nausea and vomiting in the third trimester (after 28 weeks) that is new or worsening
- Reduced foetal movements — always warrants urgent assessment, particularly in a high-risk pregnancy
- Shortness of breath or difficulty breathing
Any of these symptoms warrant same-day or emergency assessment — not a wait-and-see approach. In the context of pre-eclampsia, delay can be lethal.
Risk Factors for Pre-Eclampsia
While pre-eclampsia can occur in any pregnancy, certain factors significantly increase the risk:
- First pregnancy — over 70% of pre-eclampsia cases occur in primigravid women
- Previous pre-eclampsia — risk of recurrence in subsequent pregnancies
- Multiple pregnancy (twins, triplets)
- Chronic hypertension
- Diabetes (Type 1, Type 2, or gestational)
- Renal disease
- Autoimmune conditions — SLE, antiphospholipid syndrome
- Obesity (BMI above 30)
- Advanced maternal age (above 35)
- IVF pregnancy
- Family history of pre-eclampsia
- Interval of more than 10 years between pregnancies (long inter-pregnancy interval)
Prevention: Low-Dose Aspirin
Low-dose aspirin (75 to 150 mg/day, taken at night from 12 weeks of gestation) is the most evidence-based intervention for reducing pre-eclampsia risk in high-risk women. Multiple large trials, including the ASPRE trial, demonstrate approximately 60 to 70% risk reduction in early-onset pre-eclampsia when aspirin is started before 16 weeks in women identified as high-risk by first-trimester combined screening.
High-risk women (two or more moderate risk factors, or any high-risk factor) should be prescribed low-dose aspirin from 12 weeks. This simple, cheap, and safe medication significantly reduces the risk of the most severe pre-eclampsia. It is a critically important intervention that is still underused in India.
Monitoring During Pregnancy
Blood pressure monitoring at every antenatal appointment is the most basic and most important monitoring tool for pre-eclampsia. Urine protein testing (dipstick at each visit, quantified if positive) complements blood pressure measurement. For women at high risk, additional monitoring may include:
- More frequent appointments — fortnightly or weekly in the third trimester
- Uterine artery Doppler at 20 to 24 weeks — elevated pulsatility index predicts placental dysfunction and pre-eclampsia risk
- Foetal growth scans every 4 weeks from 28 weeks
- Serum uric acid, liver enzymes, and platelet count — if pre-eclampsia is developing
Treatment: Delivery Is the Definitive Cure
Pre-eclampsia is cured by delivery of the placenta — which removes the source of the pathological signal. All antenatal management is supportive, aimed at controlling blood pressure, preventing seizures, and buying time for foetal maturity before delivery becomes unavoidable.
- Antihypertensive medication: To control severe hypertension (above 160/110 mmHg) and reduce the risk of stroke. Oral labetalol, nifedipine, or IV hydralazine/labetalol for severe hypertension.
- Magnesium sulphate: The most important treatment for preventing eclamptic seizures — administered IV or IM in women with severe pre-eclampsia or as immediate treatment for eclampsia.
- Corticosteroids: If preterm delivery is anticipated, betamethasone or dexamethasone accelerates foetal lung maturity, significantly improving neonatal outcomes.
- Delivery timing: Depends on gestation and severity. Mild pre-eclampsia at term (37 weeks) is managed by delivery. Severe features require delivery even at earlier gestations.
Frequently Asked Questions
Q1. I had pre-eclampsia in my first pregnancy. What can I do differently in my second?
Start low-dose aspirin at 12 weeks — this is your most evidence-based risk-reduction tool. Attend antenatal appointments more frequently than in a standard pregnancy. Have uterine artery Doppler at 20 to 24 weeks to assess placental flow. Optimise any modifiable risk factors before conception (blood pressure control, weight management, thyroid treatment). Early involvement of a high-risk obstetrician is essential.
Q2. My blood pressure was 130/85 at my last antenatal visit. Should I be worried?
130/85 is elevated above the normal range for pregnancy (target below 130/80 in pregnancy in most guidelines) but not yet in the hypertensive range (140/90). It warrants more frequent monitoring — ideally every 1 to 2 weeks. A single reading should be confirmed on repeat before conclusions are drawn. If it persists or rises, investigation for early pre-eclampsia (urine protein, bloods) is appropriate.
Q3. Can pre-eclampsia develop after delivery?
Yes — postpartum pre-eclampsia occurs in approximately 25% of pre-eclampsia cases, typically within 48 hours of delivery but occasionally up to 6 weeks postpartum. New-onset severe headache, visual disturbances, or significantly elevated blood pressure in the first 6 weeks postpartum should prompt urgent assessment. This is an important and underrecognised presentation.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Every pregnancy is unique. Please consult Dr. Sunita Tandulwadkar or your qualified obstetrician for personalised guidance. Solo Clinic IVF & ObGyn, Pune.