Ectopic Pregnancy: Warning Signs, Diagnosis, and Treatment
Ectopic pregnancy — a pregnancy implanting outside the uterus, almost always in a fallopian tube — is a medical emergency. When a tubal ectopic is left untreated, the growing pregnancy eventually ruptures the tube, causing life-threatening internal haemorrhage. In India, ectopic pregnancy remains a significant cause of maternal mortality — largely preventable when recognised and treated promptly.
Every woman who is pregnant, or who might be pregnant, should know the warning signs of ectopic pregnancy. A 15-minute read of this article could save a life.
What Is an Ectopic Pregnancy?
A normal pregnancy implants in the uterine cavity. An ectopic pregnancy implants somewhere else. The most common site — approximately 95% of ectopic pregnancies — is the fallopian tube (tubal ectopic). Less commonly, ectopic implantation occurs in the ovary, the cervix, a previous caesarean scar (scar ectopic — an increasingly recognised entity in India due to high caesarean rates), or the abdominal cavity.
Regardless of location, an ectopic pregnancy cannot develop into a viable baby. The tube or other implantation site does not have the capacity to support and expand with a growing pregnancy. The growing trophoblastic tissue erodes blood vessels, causing bleeding — initially contained, eventually catastrophic if the tube ruptures.
Who Is at Risk?
Any woman of reproductive age who is sexually active can have an ectopic pregnancy. However, certain factors significantly increase the risk:
- Previous ectopic pregnancy: The single most important risk factor — the risk of recurrence is approximately 10 to 15% per subsequent pregnancy.
- Previous pelvic inflammatory disease (PID): Chlamydia and gonorrhoea infections that damage and scar the fallopian tubes are the most common cause of tubal ectopic pregnancies in India.
- Previous tubal surgery: Including previous salpingotomy (opening a tube) for a prior ectopic, or any other tubal operation.
- IVF with embryo transfer: The embryo can migrate from its transfer site into the tube. Ectopic rate in IVF is approximately 2 to 5% — higher than natural conception rate but lower than might be expected given that tubal factor infertility underlies many IVF cases.
- Previous abdominal or pelvic surgery: Adhesions can distort the tubes.
- Endometriosis: Peritubal adhesions impair embryo transit.
- IUCD (intrauterine contraceptive device) in situ: Prevents intrauterine implantation but not tubal implantation — ectopic risk is elevated relative to natural conception without contraception.
- Smoking: Associated with impaired tubal ciliary function and elevated ectopic risk.
- Advancing maternal age
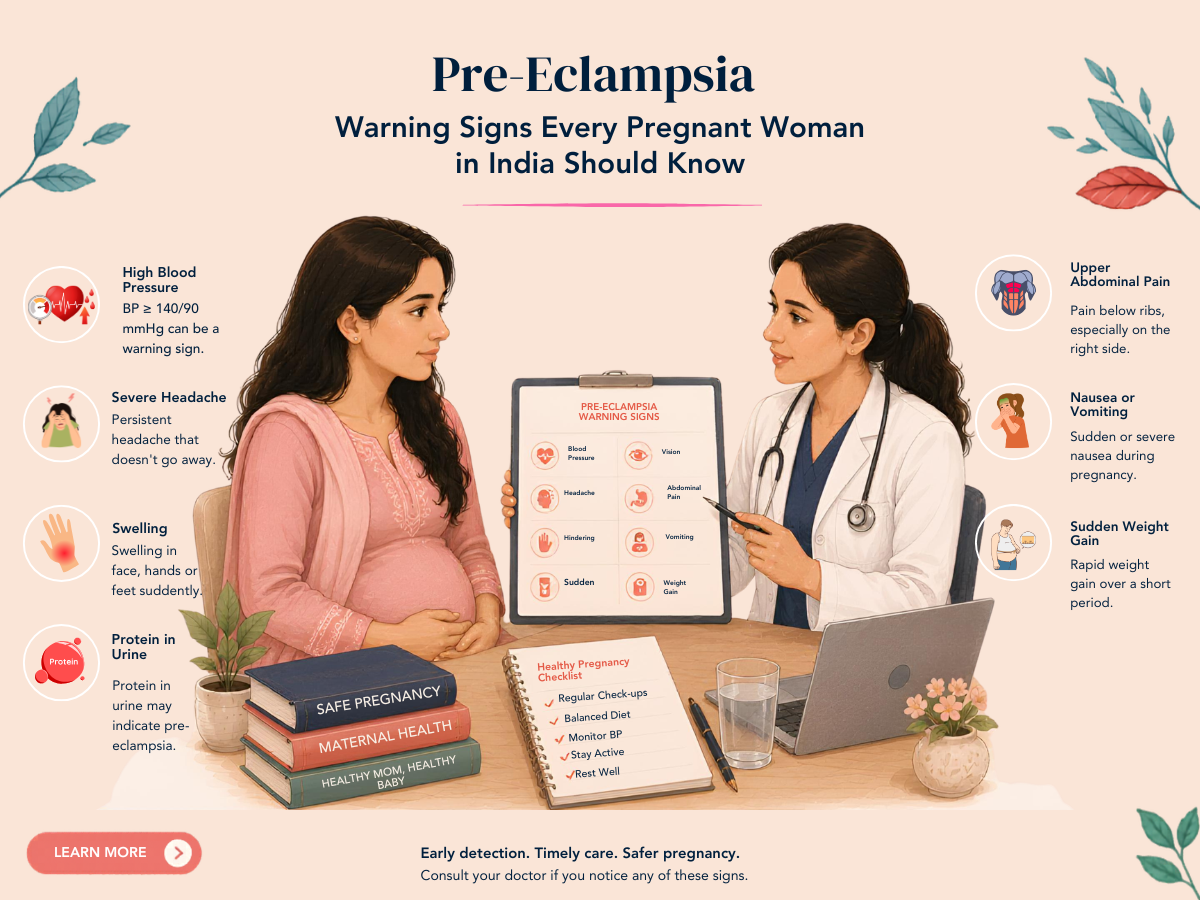
Warning Signs of Ectopic Pregnancy
The classic triad of ectopic pregnancy is: missed period + abdominal pain + vaginal bleeding. However, presentation is highly variable — ectopic pregnancies can be silent until rupture, or can present with any combination of the following:
- Positive pregnancy test with pelvic or abdominal pain — particularly one-sided pain
- Vaginal bleeding — usually lighter than a normal period, sometimes just spotting
- Shoulder tip pain — caused by blood irritating the diaphragm (a sign of significant internal bleeding — an emergency)
- Dizziness, fainting, or collapse — signs of significant haemorrhage and haemodynamic instability — EMERGENCY
- Nausea and vomiting alongside pelvic pain and a positive test
Critical rule: Any woman with a positive pregnancy test and pelvic pain should be assessed urgently for ectopic pregnancy — not reassured and sent home. A ruptured ectopic can kill within hours of symptom onset if not recognised and treated.
Diagnosis
Ectopic pregnancy is diagnosed by combining:
- Beta-hCG: A positive pregnancy test confirms pregnancy. Serial beta-hCG measurements (48 hours apart) help interpret ultrasound findings — a slow-rising or falling beta-hCG with no intrauterine sac visible suggests ectopic.
- Transvaginal ultrasound: The primary diagnostic tool. A viable intrauterine pregnancy (visible gestational sac in the uterus) effectively excludes a co-existing ectopic in most cases. An empty uterus with a positive test, or an adnexal mass separate from the ovary, suggests ectopic. A tubal ring with cardiac activity confirms it.
- Haemodynamic assessment: Blood pressure, pulse rate, and clinical signs of haemorrhage determine urgency.
Treatment Options
Expectant Management
For confirmed ectopic pregnancies with very low and falling beta-hCG (typically below 1,000 to 1,500 mIU/ml), small size on ultrasound, and no symptoms — a proportion will resolve spontaneously without treatment. This requires very close surveillance (twice-weekly beta-hCG, weekly ultrasound) and immediate access to emergency surgery if symptoms develop. Not appropriate for all patients — requires careful selection.
Medical Treatment — Methotrexate
Methotrexate (an antimetabolite medication given as a single or double injection) kills the rapidly dividing trophoblastic cells of the ectopic pregnancy, allowing the body to reabsorb it over 4 to 8 weeks. Appropriate when the ectopic is unruptured, beta-hCG is below approximately 5,000 mIU/ml (some centres use higher thresholds), there are no signs of rupture, and the patient is haemodynamically stable. Requires follow-up beta-hCG monitoring until levels reach zero, and avoidance of pregnancy for 3 months afterward (methotrexate has foetal teratogenic potential in subsequent conceptions).
Surgical Treatment
Surgery is the definitive treatment for ruptured ectopics (emergency) and for cases where medical management is inappropriate or has failed. The approach is almost always laparoscopic:
- Salpingotomy: Opening the tube and removing the ectopic while preserving the tube. Considered when the other tube is absent or damaged and tubal preservation is important for future natural fertility. Associated with higher risk of persistent trophoblast (incompletely resolved ectopic) — requires follow-up beta-hCG.
- Salpingectomy: Removing the affected tube entirely. Standard when the other tube is healthy, in cases of recurrent ectopic in the same tube, or when haemostasis is difficult. Eliminates the risk of recurrent ectopic in that tube and is associated with lower persistent trophoblast rates.
Frequently Asked Questions
Q1. I had an ectopic in my right tube. Can I still get pregnant naturally?
If your left tube is healthy, natural conception is possible — ovulation alternates between ovaries (approximately), and a pregnancy can implant normally when the egg from the healthy side is fertilised. However, the risk of a second ectopic in the remaining tube is elevated if there is any underlying tubal damage. A fertility assessment after recovery is advisable, and IVF — which bypasses the tubes — may be the most efficient approach.
Q2. I am having IVF. Can I still have an ectopic?
Yes — despite the embryo being placed directly into the uterine cavity, it can migrate into the tube in the early post-transfer period. IVF ectopic rates are approximately 2 to 5%. This is why serial beta-hCG and early ultrasound confirmation of intrauterine location are standard after a positive IVF pregnancy test. Reporting any pelvic pain promptly after a positive test is essential.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Every pregnancy is unique. Please consult Dr. Sunita Tandulwadkar or your qualified obstetrician for personalised guidance. Solo Clinic IVF & ObGyn, Pune.