Twin Pregnancy Care in Pune: What's Different and What to Expect
Twin pregnancy is exciting — but it is also significantly more complex than singleton pregnancy. The risks of preterm birth, foetal growth restriction, pre-eclampsia, gestational diabetes, anaemia, and perinatal complications are all substantially higher in twins than in singleton pregnancies. For IVF-conceived twins — which represent a significant proportion of twin pregnancies in urban India — the complexity begins even before the first antenatal appointment.
Understanding what makes twin pregnancy different, what monitoring is needed, and what to expect at each stage is the foundation of safe twin pregnancy management.
Types of Twin Pregnancy: Why Chorionicity Matters
Not all twin pregnancies are the same. The most critical classification is chorionicity — whether the twins share a placenta — because this determines the specific risks and the intensity of monitoring required.
Dichorionic-Diamniotic (DCDA) Twins
Each twin has its own placenta and its own amniotic sac. This is the less complex twin type — equivalent to two separate singleton pregnancies in the same uterus. DCDA twins are always the case with non-identical (fraternal) twins, and are also the case with identical twins who divided very early (within 3 days of fertilisation). Approximately 70 to 75% of twins are DCDA.
Monitoring schedule: Ultrasound every 4 weeks from 16 weeks to assess growth and amniotic fluid in each sac.
Monochorionic-Diamniotic (MCDA) Twins
Identical twins sharing a single placenta but each in their own amniotic sac. These arise when the fertilised egg divides between days 4 and 8. The shared placenta creates a specific risk: twin-to-twin transfusion syndrome (TTTS), in which blood is transferred unevenly from one twin (the "donor") to the other (the "recipient"), causing the donor to become anaemic and growth-restricted while the recipient develops cardiac overload. TTTS occurs in approximately 10 to 15% of MCDA pregnancies and can be rapidly progressive.
Monitoring schedule: Every 2 weeks from 16 weeks to 26 weeks for TTTS surveillance; then every 4 weeks thereafter.
Monochorionic-Monoamniotic (MCMA) Twins
Sharing both a placenta and an amniotic sac — the highest-risk twin type, arising when division occurs after day 8. Risk of cord entanglement and acute foetal compromise is significant. These pregnancies require management at a specialist foetal medicine centre with planned admission and delivery before 34 weeks.
Key Risks in Twin Pregnancy
Preterm Birth
The most significant risk in twin pregnancy. Spontaneous preterm birth before 37 weeks occurs in approximately 50 to 60% of twin pregnancies; preterm birth before 32 weeks occurs in approximately 10 to 15%. The mechanisms include uterine overdistension, cervical shortening, and placental insufficiency.
Monitoring: Cervical length measurement at 20 to 24 weeks. A short cervix (below 25 mm) in twin pregnancy is associated with significantly elevated preterm risk and may prompt discussion of vaginal progesterone or cervical cerclage.
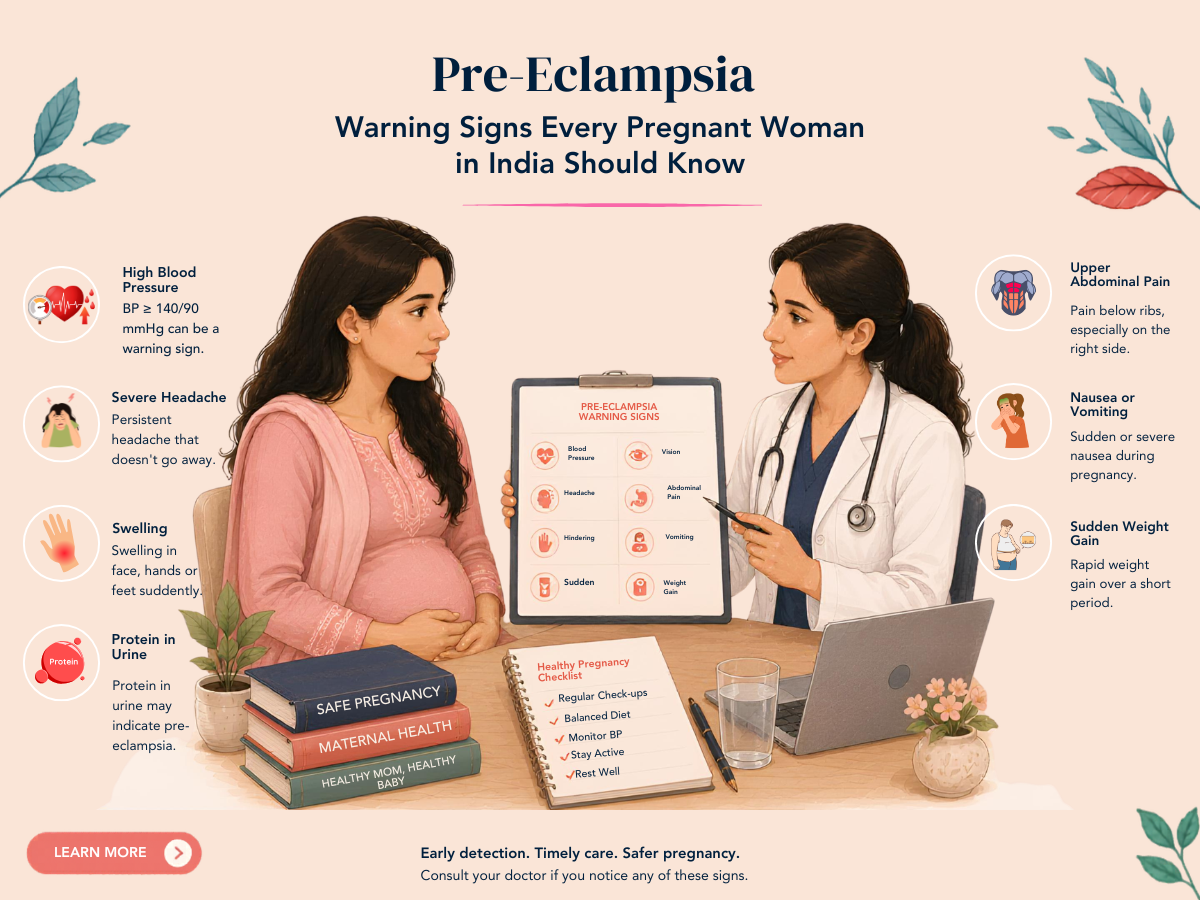
Pre-Eclampsia
Approximately 3 to 5 times more common in twin pregnancies than singletons, and tends to occur earlier and be more severe. Low-dose aspirin from 12 to 16 weeks, regular blood pressure monitoring, and close urine surveillance are standard.
Twin-to-Twin Transfusion Syndrome (TTTS)
Affecting only MCDA twins. Classified in stages (Quintero I to V) based on severity. Mild cases may resolve spontaneously or progress slowly. Severe TTTS (Stage III to V) requires intervention — fetoscopic laser photocoagulation of the vascular communications on the placenta, performed at a specialist foetal medicine centre. Without treatment, severe TTTS has very high foetal mortality in both twins.
Selective Foetal Growth Restriction (sFGR)
One twin receiving significantly less placental territory than the other, resulting in growth discordance. Requires intensive Doppler surveillance. Depending on severity, management ranges from close observation to delivery.
Anaemia
Twin pregnancies have significantly higher iron requirements than singleton pregnancies. Iron deficiency anaemia is common and should be actively screened for and treated throughout pregnancy.
Gestational Diabetes
More common in twin pregnancies — GDM screening is essential.
The Twin Pregnancy Monitoring Schedule
DCDA twins: Ultrasound every 4 weeks from 16 weeks; growth and Doppler from 28 weeks; antenatal appointments every 2 to 4 weeks; cervical length at 20 to 24 weeks.
MCDA twins: Ultrasound every 2 weeks from 16 weeks to 26 weeks (for TTTS); then every 4 weeks; more frequent monitoring if TTTS or sFGR develops.
All twin pregnancies: OGTT at 24 to 28 weeks (or earlier if PCOS/risk factors), iron studies every 4 weeks, blood pressure monitoring at every visit, foetal movements tracking from 28 weeks.
Delivery Planning for Twin Pregnancies
The optimal timing and mode of delivery in twin pregnancy depends on chorionicity and foetal presentation:
- DCDA twins with both presenting head-down (cephalic): Vaginal delivery is generally possible if labour proceeds normally and the hospital has appropriate twin delivery experience. Delivery is usually planned at 37 to 38 weeks.
- DCDA twins with first twin presenting head-down and second in breech: May attempt vaginal delivery at experienced centres. Requires willingness and expertise to perform internal podalic version or breech delivery of the second twin.
- MCDA twins: Planned delivery at 36 to 37 weeks (earlier if TTTS or sFGR). Mode depends on presentation.
- Any twin pregnancy where the first twin is breech: Caesarean section is standard.
Frequently Asked Questions
Q1. I am expecting IVF twins. Should I reduce to a singleton?
Multifetal pregnancy reduction — reducing a twin pregnancy to a singleton — is a difficult personal decision with medical, ethical, and emotional dimensions. It reduces the risk of preterm birth and associated neonatal complications significantly, but involves a procedure with its own small risk of complete pregnancy loss. The decision depends on your specific circumstances, gestational age of discovery, and personal values. A detailed discussion with your fertility specialist and foetal medicine specialist is essential. Solo Clinic does not pressure couples either way — this is a decision that requires complete information and patient autonomy.
Q2. My twins are MCDA. How often do I need ultrasound?
Fortnightly ultrasound from 16 to 26 weeks is the standard for MCDA twins, to detect TTTS early enough for intervention when it develops. From 26 weeks, the major TTTS risk has passed (because after this gestation, laser intervention is no longer safe and delivery would be considered in severe cases). After 26 weeks, monthly growth scans and regular Doppler surveillance continue.
Q3. What is the expected weight of twin babies at birth?
Twin birth weights vary widely depending on gestational age at delivery. At 37 to 38 weeks, DCDA twins typically weigh 2.2 to 2.8 kg each. Preterm twins (before 34 weeks) are smaller and require NICU support. Growth discordance (one significantly smaller than the other) requires investigation — it may reflect placental insufficiency in the growth-restricted twin.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Every pregnancy is unique. Please consult Dr. Sunita Tandulwadkar or your qualified obstetrician for personalised guidance. Solo Clinic IVF & ObGyn, Pune.