High-Risk Pregnancy Care in Pune: What It Is and When You Need It
Pregnancy is a normal physiological process — one that has occurred billions of times in human history without medical intervention. For the majority of women, pregnancy progresses safely with routine antenatal monitoring. But a significant minority — estimates range from 6 to 20% of pregnancies, depending on the definition used — involve factors that meaningfully increase the risk of complications for the mother, the baby, or both. These are high-risk pregnancies, and they deserve care that goes beyond what routine antenatal monitoring provides.
Understanding what makes a pregnancy high-risk, what specialist management looks like, and when to seek it is not about inducing fear. It is about ensuring that women who need enhanced care receive it in time — not after a complication has already occurred.
What Is a High-Risk Pregnancy?
A pregnancy is classified as high-risk when identifiable factors — present before conception, arising during pregnancy, or developing in the foetus — increase the probability of adverse outcomes for the mother, the baby, or both above the baseline risk for uncomplicated pregnancy.
This classification is a tool for directing resources and surveillance appropriately. It does not mean that every high-risk pregnancy will have a poor outcome — the majority of women with risk factors deliver healthy babies with appropriate care. What it means is that the pregnancy requires more frequent monitoring, specialist input, and sometimes earlier or more active management than a straightforward low-risk pregnancy.
Categories of High-Risk Pregnancy
Maternal Medical Conditions Pre-Dating Pregnancy
Women with pre-existing medical conditions face additional complexity in pregnancy because the physiological changes of pregnancy — increased blood volume, altered cardiac output, metabolic shifts, immune modulation — interact with and sometimes worsen underlying disease:
- Diabetes mellitus (Type 1 or Type 2): Pre-existing diabetes significantly increases risk of foetal congenital anomalies (particularly cardiac and neural tube defects), macrosomia (large baby), shoulder dystocia, operative delivery, and perinatal complications. Tight glycaemic control before and throughout pregnancy is the most important modifiable factor.
- Hypertension: Pre-existing hypertension elevates risk of superimposed pre-eclampsia, placental abruption, foetal growth restriction, and preterm delivery. Antihypertensive medications must be reviewed before conception — some (ACE inhibitors, ARBs) are contraindicated in pregnancy and need switching.
- Thyroid disorders: Both hypothyroidism and hyperthyroidism require careful monitoring and dose adjustment throughout pregnancy. Untreated thyroid disease increases risk of miscarriage, foetal neurological development problems, and preterm birth.
- Cardiac disease: Women with congenital or acquired heart disease require cardio-obstetric co-management. The increased cardiac demands of pregnancy (40% increase in blood volume by mid-pregnancy) can destabilise compensated cardiac conditions.
- Autoimmune conditions: Lupus (SLE), antiphospholipid syndrome, and other autoimmune disorders significantly increase risk of pregnancy loss, preterm birth, and foetal growth restriction. Antiphospholipid syndrome treated with aspirin and heparin improves pregnancy outcomes substantially.
- Renal disease: Significant renal impairment is associated with elevated risk of pre-eclampsia, preterm birth, and worsening of underlying kidney disease during pregnancy.
- Epilepsy: Anti-epileptic medications require review before conception — some are teratogenic. Seizure control during pregnancy is critical for maternal and foetal safety.
Obstetric History Risk Factors
Previous pregnancy complications predict elevated risk in subsequent pregnancies:
- Previous preterm birth (before 37 weeks): The most significant predictor of recurrent preterm delivery. Women with a history of spontaneous preterm birth benefit from cervical length surveillance, progesterone supplementation, and sometimes cervical cerclage.
- Previous severe pre-eclampsia or HELLP syndrome: Elevates risk of recurrence in subsequent pregnancies. Low-dose aspirin from early pregnancy reduces recurrence risk.
- Previous caesarean section: Relevant for uterine scar assessment, risk of placenta praevia, placenta accreta spectrum, and decisions about delivery mode.
- Recurrent pregnancy loss: Indicates need for thrombophilia screening, antiphospholipid antibody testing, and enhanced early pregnancy surveillance.
- Previous stillbirth: Requires detailed investigation of the cause and enhanced foetal surveillance in a subsequent pregnancy.
- Previous shoulder dystocia or severe PPH: Informs delivery planning in subsequent pregnancies.
Current Pregnancy Risk Factors
Conditions developing during the current pregnancy that confer high-risk status:
- Gestational diabetes: Develops in approximately 12 to 18% of Indian pregnancies. Requires dietary management, blood glucose monitoring, sometimes insulin or oral medication, and enhanced foetal surveillance for macrosomia.
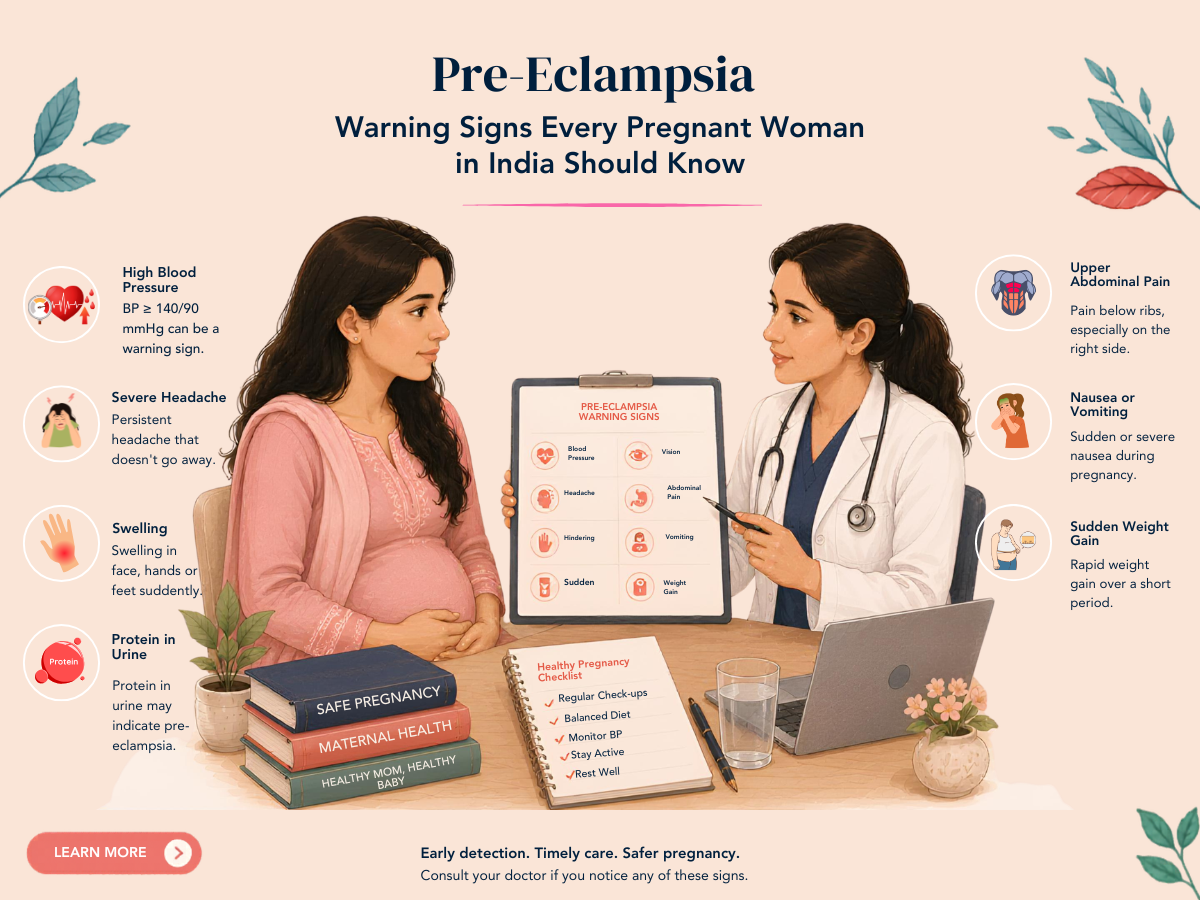
- Pre-eclampsia: Hypertension developing after 20 weeks with proteinuria or end-organ features. Requires close monitoring and sometimes early delivery to prevent maternal and foetal complications.
- Multiple pregnancy (twins or more): Significantly elevated rates of preterm birth, growth discordance, twin-to-twin transfusion syndrome (for monochorionic twins), and maternal complications.
- Foetal growth restriction (FGR): A baby growing below the 10th centile for gestation, particularly with abnormal umbilical artery Doppler flow — indicates placental insufficiency and requires intensive surveillance.
- Placenta praevia: Placenta overlying or near the cervix — associated with antepartum haemorrhage and requires caesarean delivery.
- Placental abruption: Separation of the placenta before delivery — a pregnancy emergency.
- Polyhydramnios or oligohydramnios: Abnormal amniotic fluid volumes associated with foetal anomalies or placental dysfunction.
Advanced Maternal Age
Women aged 35 and above at delivery have incrementally higher risks of chromosomal conditions (trisomy 21 particularly), gestational diabetes, hypertension, placental complications, and stillbirth. These risks increase further above 40. Enhanced surveillance is appropriate from 35 onward; more intensive monitoring from 40.
IVF and Assisted Conception Pregnancies
IVF-conceived pregnancies carry modestly elevated rates of pre-eclampsia, placenta praevia, preterm birth, and foetal growth restriction compared to naturally conceived singleton pregnancies. The reasons are incompletely understood. All IVF pregnancies should receive high-risk antenatal monitoring regardless of otherwise low-risk profiles.
What High-Risk Antenatal Care Looks Like
High-risk antenatal care differs from routine care in frequency, depth of surveillance, and the involvement of specialist expertise:
- More frequent appointments: Instead of monthly visits in the second trimester and fortnightly in the third, high-risk pregnancies may be reviewed every 2 to 4 weeks throughout, with weekly monitoring in the third trimester for conditions like FGR or severe hypertension.
- Additional ultrasound surveillance: Growth scans every 4 weeks for FGR, cervical length measurement at 20 to 24 weeks for preterm risk assessment, Doppler blood flow assessment of umbilical and uterine arteries.
- Specialist consultations: Cardiology, nephrology, endocrinology, neonatology, or other specialties depending on the specific risk.
- Non-invasive prenatal testing (NIPT): Chromosomal screening from 10 weeks, particularly appropriate for advanced maternal age and IVF pregnancies.
- Enhanced gestational diabetes screening: OGTT at 24 to 28 weeks as standard, or earlier in high-risk women (prior GDM, strong family history, obesity, PCOS, previous macrosomic baby).
- Planned delivery timing: Many high-risk conditions require planned delivery before 40 weeks — the optimal timing is condition-specific and requires specialist judgment.
- Delivery location planning: Women with significant cardiac disease, severe pre-eclampsia, or extreme prematurity should be delivered at a centre with appropriate NICU and specialist backup.
High-Risk Obstetric Care at Solo Clinic
Dr. Sunita Tandulwadkar provides comprehensive high-risk obstetric management with continuity from fertility treatment through delivery — ensuring that patients who conceived through IVF at Solo Clinic receive the specialist antenatal oversight their pregnancy requires. Key capabilities include:
- Comprehensive antenatal assessment from the first positive pregnancy test
- Integrated management of IVF pregnancies, twin pregnancies, and pregnancies with pre-existing medical conditions
- Cervical length surveillance and progesterone for preterm prevention
- Close gestational diabetes screening and management — including insulin protocols where needed
- Pre-eclampsia risk stratification and aspirin prophylaxis protocols
- Detailed foetal surveillance — growth scans, Doppler, biophysical profile
- Coordination with neonatology for planned preterm deliveries
Frequently Asked Questions
Q1. Does being high-risk mean I will definitely have complications?
No. High-risk classification means your probability of a complication is elevated above baseline — not that a complication is inevitable. The majority of women with high-risk pregnancies, when managed appropriately, deliver healthy babies. The purpose of high-risk care is precisely to identify and manage threats before they become crises.
Q2. I had a normal first pregnancy. Can my second be high-risk?
Yes — conditions can develop for the first time in any pregnancy. Gestational diabetes, pre-eclampsia, and placental problems can occur in a second or third pregnancy even if the first was entirely uncomplicated. A fresh baseline assessment at the beginning of each pregnancy is appropriate regardless of previous history.
Q3. My first baby was premature. What can be done to prevent it happening again?
Several evidence-based interventions reduce recurrent preterm birth risk in women with a previous spontaneous preterm delivery: cervical length surveillance from 16 weeks (cervical length below 25 mm at 20 to 24 weeks is a strong risk marker), vaginal progesterone supplementation, and cervical cerclage (a stitch to reinforce the cervix) in selected cases. The specific approach depends on the gestational age of the previous delivery and whether the preterm birth was spontaneous or provider-initiated.
Q4. When should I start seeing a high-risk obstetrician?
Ideally before conception — a preconception consultation allows risk stratification and medication review before pregnancy begins. For women who are already pregnant and have a known risk factor, the first trimester is the right time. For conditions developing during pregnancy (gestational diabetes, hypertension), referral should happen as soon as the condition is identified.
Q5. Can I have a vaginal delivery with a high-risk pregnancy?
In many cases, yes. High-risk status does not automatically mean caesarean delivery. The mode of delivery depends on the specific risk factors, foetal presentation, and the progression of the pregnancy and labour. Conditions like placenta praevia, foetal distress, or certain severe maternal conditions may require caesarean. But many women with high-risk pregnancies — including twins in appropriate presentations, IVF pregnancies, and women with well-controlled medical conditions — deliver vaginally.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Every pregnancy is unique. Please consult Dr. Sunita Tandulwadkar or your qualified obstetrician for personalised guidance. Solo Clinic IVF & ObGyn, Pune.