What Makes a Pregnancy High-Risk? A Complete List of Factors
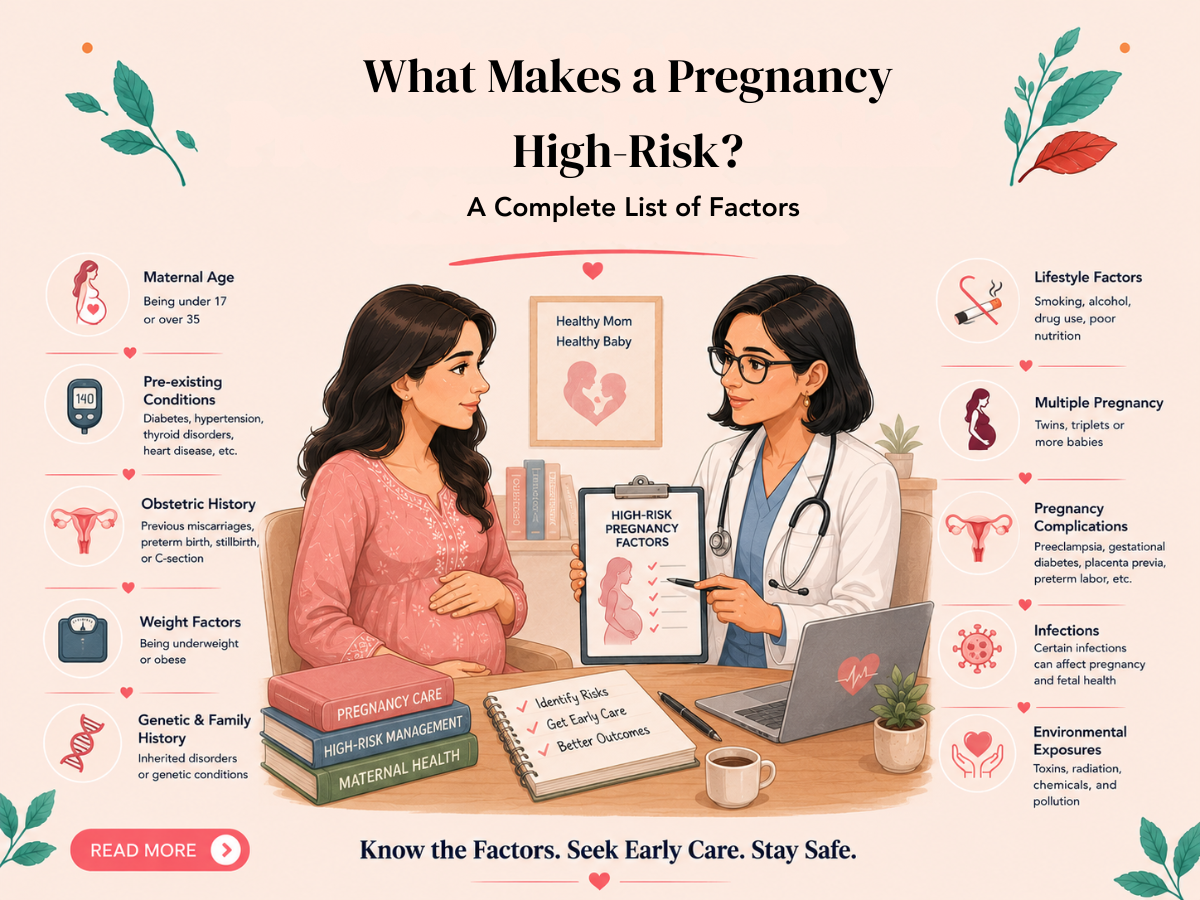
High-risk pregnancy is not a single diagnosis — it is a classification that applies to any pregnancy where the probability of adverse outcomes is meaningfully elevated above the baseline. Understanding which specific factors confer high-risk status — and what each one means for antenatal management — helps pregnant women make informed decisions about the level and type of care they seek.
This article provides a comprehensive reference list of high-risk pregnancy factors, grouped by category, with brief notes on the clinical significance of each.
Maternal Age
- Under 18: Adolescent pregnancy is associated with elevated rates of anaemia, pre-eclampsia, preterm birth, and low birth weight, partly due to the physiological immaturity of the young mother's body and partly due to associated socioeconomic factors.
- 35 to 39 at delivery: Increased risk of gestational diabetes, hypertension, chromosomal conditions (Down syndrome), placenta praevia, and stillbirth. Incremental but meaningful above the 35-year threshold.
- 40 and above: All the above risks are further elevated. The absolute risk of stillbirth in women 40 and above is approximately double that of women aged 25 to 29. Close surveillance from 36 to 37 weeks, including consideration of delivery by 39 to 40 weeks, is standard practice in many guidelines.
Pre-Existing Maternal Medical Conditions
- Type 1 or Type 2 diabetes: Pre-conception glycaemic control is the most important modifiable factor. HbA1c below 6.5% before conception reduces the risk of congenital anomalies toward background rates. Ongoing close glucose monitoring, insulin adjustment, and foetal surveillance throughout pregnancy are essential.
- Hypertension: Target blood pressure in pregnancy is below 140/90 mmHg. Antihypertensive medications must be pregnancy-safe — labetalol, methyldopa, and nifedipine are the main agents used in Indian practice. ACE inhibitors and ARBs must be stopped before conception.
- Thyroid disorders: Both hypothyroidism (TSH above 2.5 mIU/L in the first trimester) and hyperthyroidism require treatment and monitoring. Untreated hypothyroidism in early pregnancy is associated with impaired foetal neurological development.
- Cardiac disease: Congenital heart disease, valvular disease, cardiomyopathy. All require cardio-obstetric co-management. Specific lesions carry specific risks — some women with severe cardiac disease are counselled that pregnancy carries life-threatening risk.
- Systemic lupus erythematosus (SLE): Associated with lupus nephritis flares, foetal heart block (from anti-Ro/La antibodies), foetal growth restriction, and preterm birth. Requires rheumatology and obstetric co-management.
- Antiphospholipid syndrome: Causes recurrent pregnancy loss and second/third trimester foetal loss through placental thrombosis. Treatable — aspirin + heparin significantly improves outcomes.
- Renal disease: Elevated creatinine and proteinuria before pregnancy are associated with worsening renal function during pregnancy and significantly elevated pre-eclampsia risk.
- Epilepsy: Requires anticonvulsant review before conception. Valproate is contraindicated in pregnancy due to severe teratogenicity — women of reproductive age should not receive valproate without very specific justification and robust contraception.
- Haemoglobinopathies: Sickle cell disease, thalassaemia major, and other severe haemoglobin disorders require specialist haematology-obstetric co-management.
- Severe obesity (BMI above 40): Associated with gestational diabetes, pre-eclampsia, sleep apnoea, increased caesarean rate, wound complications, and VTE (blood clot) risk.
- HIV and hepatitis: Require specialist management to minimise vertical transmission to the baby and to ensure maternal health during pregnancy.
Obstetric History
- Previous preterm birth (spontaneous, below 34 weeks): The single strongest predictor of recurrent preterm birth. Short cervix on surveillance adds further risk.
- Previous stillbirth: Requires detailed investigation of cause; growth and Doppler surveillance from 26 to 28 weeks in subsequent pregnancy; planned delivery by 38 to 40 weeks depending on cause.
- Recurrent pregnancy loss (two or more consecutive): Requires thrombophilia and antiphospholipid antibody evaluation; enhanced early pregnancy surveillance.
- Previous severe pre-eclampsia or HELLP syndrome: Low-dose aspirin (75 to 150 mg/day) from 12 weeks reduces recurrence risk by approximately 10 to 20%.
- Previous caesarean section: Uterine scar integrity should be assessed; placenta praevia/accreta risk is elevated with increasing number of prior caesareans. Trial of labour after caesarean (VBAC) may be discussed in appropriate cases.
- Previous third or fourth degree perineal tear: Relevant for delivery planning in subsequent pregnancies.
- Previous PPH (postpartum haemorrhage): Managed delivery with oxytocin prophylaxis, IV access, and blood product availability on standby.
Current Pregnancy Complications
- Multiple pregnancy (twins, triplets): Elevated rates of preterm birth, TTTS (twin-to-twin transfusion syndrome in monochorionic twins), growth discordance, anaemia, pre-eclampsia, and maternal discomfort. Monochorionic twins require fortnightly scans from 16 weeks.
- Gestational diabetes: Develops in 12 to 18% of Indian pregnancies. See dedicated article for full management.
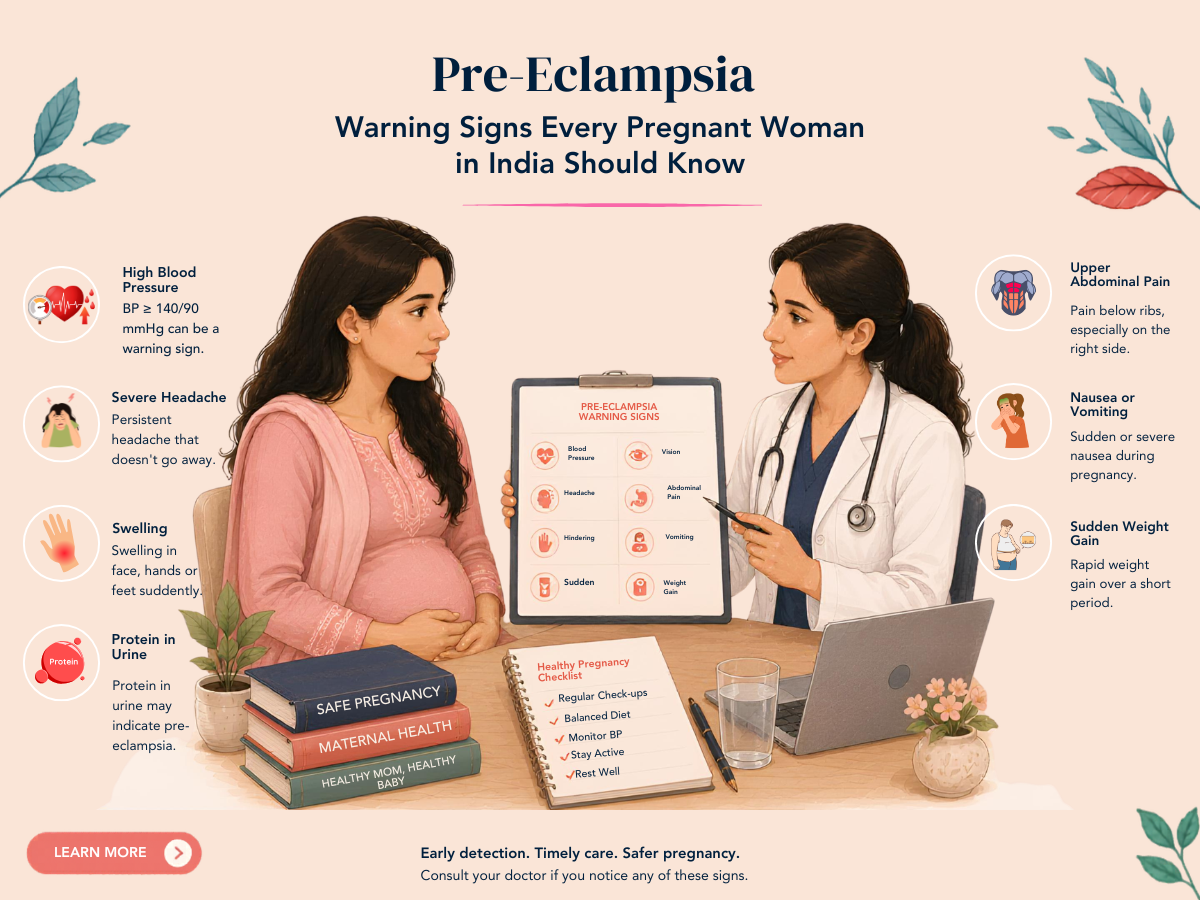
- Pre-eclampsia: Hypertension plus proteinuria or end-organ features after 20 weeks. See dedicated article.
- Foetal growth restriction (FGR): Estimated foetal weight below 10th centile, particularly with abnormal Doppler. Requires intensive surveillance and timed delivery.
- Placenta praevia (major): Placenta covering the internal cervical os. Requires caesarean delivery and high-volume bleeding preparedness.
- Placenta accreta spectrum: Abnormal placental implantation into or through the myometrium. Higher risk with prior caesareans. Planned delivery at a specialist centre with haematological backup.
- Vasa praevia: Foetal blood vessels crossing the cervical os — associated with catastrophic foetal haemorrhage at membrane rupture. Diagnosed by colour Doppler; planned caesarean before labour.
- Polyhydramnios: Excess amniotic fluid — associated with foetal swallowing abnormalities, neural tube defects, and diabetes.
- Oligohydramnios: Reduced amniotic fluid — associated with foetal renal abnormalities, placental insufficiency, and post-dates pregnancy.
- Threatened preterm labour: Contractions with cervical change before 37 weeks. Requires assessment, tocolysis if appropriate, corticosteroids for foetal lung maturation, and transfer to a centre with NICU.
Foetal Factors
- Confirmed chromosomal abnormality: Down syndrome, Turner syndrome, and other aneuploidies require specialist genetic counselling and enhanced foetal surveillance.
- Structural foetal anomaly: Cardiac defects, neural tube defects, abdominal wall defects, and other anomalies require foetal medicine input and delivery planning at an appropriate centre.
- Reduced foetal movements: Perceived reduction in foetal movements after 28 weeks warrants urgent assessment — it is one of the most important warning signs of foetal compromise.
Frequently Asked Questions
Q1. I am 36, otherwise healthy, and pregnant for the first time. Am I high-risk?
Advanced maternal age (35 and above) does confer somewhat elevated risk — particularly for chromosomal conditions, gestational diabetes, and hypertensive complications. This warrants a few additional measures: NIPT or combined first trimester screening for chromosomal risk, OGTT at 24 to 28 weeks for gestational diabetes, and perhaps closer blood pressure monitoring. But it does not necessarily mean intensive specialist-only management — most women in their mid-to-late thirties who are otherwise healthy progress through pregnancy with close but not dramatically different monitoring from younger women.
Q2. I have well-controlled asthma. Is my pregnancy high-risk?
Mild to moderate well-controlled asthma in pregnancy is generally associated with good outcomes when medication is continued appropriately (most asthma inhalers are safe in pregnancy). Poorly controlled asthma — with frequent exacerbations — is associated with elevated risk of pre-eclampsia, preterm birth, and low birth weight. The key is not to stop asthma treatment out of concern about medications — the risk of uncontrolled asthma in pregnancy typically exceeds the risk of the medications used to treat it.
DISCLAIMER: This article is for educational purposes only and does not constitute medical advice. Every pregnancy is unique. Please consult Dr. Sunita Tandulwadkar or your qualified obstetrician for personalised guidance. Solo Clinic IVF & ObGyn, Pune.